Thoracic Outlet Syndrome

Thoracic Outlet Syndrome Anatomy
What is Thoracic Outlet Syndrome?
Thoracic outlet syndrome, is a result of compression of one part of that neurovascular bundle either the brachial plexus, the subclavian vein, the subclavian artery within that thoracic outlet.
The 3 Types of Thoracic Outlet Syndrome
1. Neurogenic
The Neurogenic type of Thoracic Outlet Syndrome accounts for 80% of cases. Compression of the nerves of brachial plexus occurs mostly at the base of the scalenii triangle area, between the first rib and the anterior and middle scalenii muscles. Compression may also occur behind pec minor in the retropectoral space. 60% of Neurogenic cases have double crush root compression at both those areas.
2. Arterial
Arterial, is the least common type and results from damage to the subclavian artery, mostly due to abnormal bony changes. 6% of patients with Neurogenic Thoracic Outlet Syndrome have a venous component to their problems.
3. Venous
Prevalence of Thoracic Outlet Syndrome
Venous Thoracic Outlet Syndrome is the result of compression of the Subclavian Vein,generally at the junction of the first rib in the clavicle.
71% of cases are female and there also seems to be an association with hypermobility.
The Criteria for diagnosis of Thoracic Outlet Syndrome

Signs of Thoracic Outlet Syndrome
The average time to diagnosis is 5 years, so many patients have had multiple investigations, treatments and surgeries that have failed. The consensus is that 3 our of the four criteria need to be met to confirm a TOS diagnosis.
Criteria One: hand & arm symptoms
Hand and arm symptoms consistent with nerve compression, often worse with activities involving either arms overhead or with arms hanging downwards. Symptoms may refer into the head, the face, upper back, scapular region, the shoulder girdle, and the anterior clavicle. Referral may also occur into the chest, the axilla, and shoulder region. Symptoms are often describe heaviness.
Criteria Two: pain & tenderness on palpation of
Scalenii Triangle or Pectoralis Minor insertion
Pain and tenderness is noted that may or may not reproduce the patient's symptoms when the either the Scalenii Triangle or Pectoralis Minor insertion is palpated.
Criteria Three: absence of another diagnosis
Excluding other potential sources of pain namely cervical nerve root pathology and peripheral nerve entrapments.
Cervical nerve root compression present with a more specific dermatomal and myotomal presentation, and are mainly associated findings in the cervical spine and scans of the cervical spine supporting these findings.
Cervical Brachial Symptoms Questionnaire.Cervical nerve root compression present with a more specific dermatomal and myotomal presentation, and are mainly associated findings in the cervical spine and scans of the cervical spine supporting these findings.
Criteria Four: positive response to a scalenii block or injections
Evaluation of Thoracic Outlet Syndrome: Tests & Questionnaires
1. The elevated arm EAST test or Roos test. ( 90% sensitive)
2. Upper Limb Tension Test. Bilateral shoulder abduction with the arms extended, extending the wrist and laterally flexing the neck looking to reproduce symptoms.
3. Cervical Brachial Symptoms Questionnaire and that can help you actually differentiate between cervical causes of arm symptoms and thoracic outlet
2. Upper Limb Tension Test. Bilateral shoulder abduction with the arms extended, extending the wrist and laterally flexing the neck looking to reproduce symptoms.
3. Cervical Brachial Symptoms Questionnaire and that can help you actually differentiate between cervical causes of arm symptoms and thoracic outlet
Causes of Thoracic Outlet Syndromes
Congenital Factors:
* The presence of a Cervical rib
* an elongated transverse process
* Muscle Anomalies in shape and insertions
* Fibrous anomalies
* Scoliosis in the Neck Region
* Congenital elevated scapula
* Location of Subclavian Artery or Vein in relation to the Scalene Anterior Muscle
Acquired Conditions:
* Postural factors- depressed shoulder position, poor work posture, Repetitive stress injuries
* Heavy Breast Tissue
* Trauma- Clavicle fracture, Rib fracture, Hyperextension neck injury, whiplash
Muscular Causes:
* Hypertrophy of the Scalene Muscles
* Decrease of the tone of Trapezius, Levator Scapulae, Rhomboids
* Shortening of the Scalene Trapezius, Levator Scapulae, Pectoral muscles
* The presence of a Cervical rib
* an elongated transverse process
* Muscle Anomalies in shape and insertions
* Fibrous anomalies
* Scoliosis in the Neck Region
* Congenital elevated scapula
* Location of Subclavian Artery or Vein in relation to the Scalene Anterior Muscle
Acquired Conditions:
* Postural factors- depressed shoulder position, poor work posture, Repetitive stress injuries
* Heavy Breast Tissue
* Trauma- Clavicle fracture, Rib fracture, Hyperextension neck injury, whiplash
Muscular Causes:
* Hypertrophy of the Scalene Muscles
* Decrease of the tone of Trapezius, Levator Scapulae, Rhomboids
* Shortening of the Scalene Trapezius, Levator Scapulae, Pectoral muscles
Thoracic Outlet Syndrome Symptoms
Compressors
Symptoms experienced throughout the daytime during prolonged postures which increased tension or compression of the thoracic outlet. The most common aggravating postures are head forward with the shoulder girdles protracted and depressed or activities that involve working overhead with the arms elevated.
Releasers
Paraesthesia (numbness) symptoms are experienced at night, often causing disrupted sleep. Caused by a release of tension or compression to thoracic outlet, that restores the perineural blood supply to the brachial plexus, and a return of normal sensation.
Symptoms experienced throughout the daytime during prolonged postures which increased tension or compression of the thoracic outlet. The most common aggravating postures are head forward with the shoulder girdles protracted and depressed or activities that involve working overhead with the arms elevated.
Releasers
Paraesthesia (numbness) symptoms are experienced at night, often causing disrupted sleep. Caused by a release of tension or compression to thoracic outlet, that restores the perineural blood supply to the brachial plexus, and a return of normal sensation.
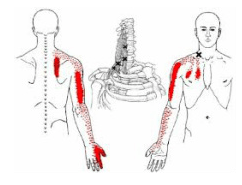
Pain Distribution for Thoracic Outlet Syndrome
Thoracic Outlet Syndrome Rehabilitation
Physiotherapy has shown to be a useful approach in 50 to 90% of all TOS cases. A six-month long program consisting of at-home exercises, stretching, postural reeducation, and retraining muscle recruitment patterns, particularly of the neck and shoulder, can improve TOS symptoms.
Initially rehabilitation incorporates strengthening of the scapular muscles (middle and lower trapezius and rhomboids and the serratus anterior) in an effort to stabilize the shoulder. along with stretching of the scalenes and pectoralis muscles. Generally horizontal adduction movements are minimised or avoided to prevent further injury. Proper technique is essential throughout the rehabilitation process with re education of breathing techniques,
and head and pelvis alignment during various tasks.
Initially rehabilitation incorporates strengthening of the scapular muscles (middle and lower trapezius and rhomboids and the serratus anterior) in an effort to stabilize the shoulder. along with stretching of the scalenes and pectoralis muscles. Generally horizontal adduction movements are minimised or avoided to prevent further injury. Proper technique is essential throughout the rehabilitation process with re education of breathing techniques,
and head and pelvis alignment during various tasks.

Basic Exercises for Thoracic Outlet Syndrome