The extra bone formation is not uncommon and may be formed in athletic populations as a normal response to loading. The individual with these bony changes may never experience hip pain if they don't engage in activity that takes them into end of range hip movements, ie. deep squats.
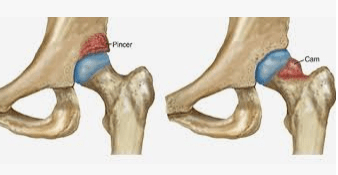
So there is no need to rush out and get your hips scanned if you don't have any other signs or symptoms. Although worth noting, CAM morphology is associated with an increased prevalence of Hip Osteoarthritis and need for hip replacement
FIA Treatment
If you are thinking that you might have FAI, what are your options?
Obviously surgery may seem like a good solution: remove the extra bit of bone and everything is good? There are not many quality studies assessing surgical effectiveness. For those under 40 years of age, with CAM morphology and not a lot else, surgical outcomes are more favourable. But the hip is not likely to feel or function like brand new again.
A minimum of 3 months of conservative management should be the aim for all patients before considering surgical options. The primary goals are to maintain or work towards a healthy body weight, develop good muscle strength around the hip and trunk area, and participate in regular cardiovascular exercise to enhance fitness and joint load tolerance.
Manual physiotherapy techniques that may be included in the process are traction, deep tissue releases, and joint mobilisations.
Flare ups are a normal course of progression for FAI rehabilitation and working towards exercise progression, functional movement patterns should be the aim of treatment.
Consider specifically strengthening the adductors primarily, the abductors, hip extensors and hip external rotators. Endurance of the trunk muscles ie. the extensors, flexors and lateral flexors, are also important as fatigue in this area may unnecessarily load the hip.
The rehabilitation process may use therabands, powerbands, weighted cuffs, resistance machines, hydrotherapy, cycling and progressive walking program as well as an inclusion of functional movement patterns.
This 3 month process is perfect preparation for surgery if that becomes the final outcome. Improved fitness, muscle strength, mobility and healthy body weight will ensure optimal surgical results.
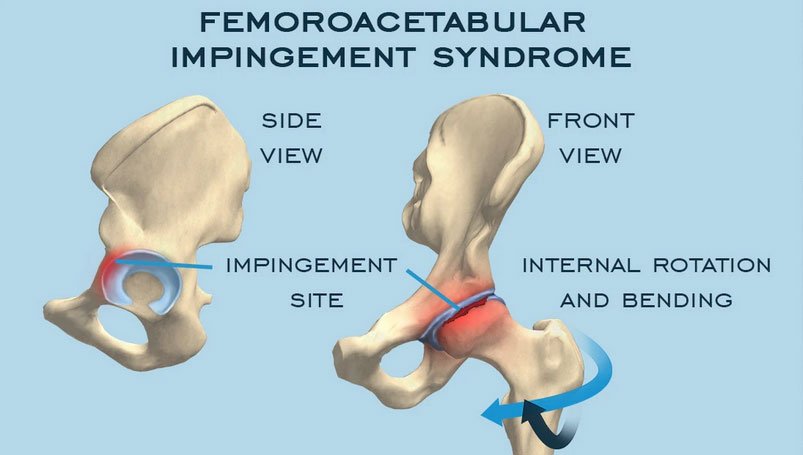
Movements which increase FIA